Introduction
Dentin/Dentinal hypersensitivity (DHS) may be defined as short, sharp pain arising from exposed dentine typically in response to chemical, thermal or osmotic stimuli that cannot be explained as arising from any other form of dental defect or pathology[1]. The two most common pathways that lead to dentin exposure and dentin hypersensitivity are gingival recession[2] and enamel loss due to abrasion, erosion, attrition and abfraction. A variety of products for home use and professional treatments for dentin hypersensitivity are available e.g., desensitizing toothpastes, mouth rinses with high fluoride content, varnishes and restorative materials etc. Many desensitizing toothpastes contain a potassium salt which is believed to work by penetrating the length of the dentinal tubule and depolarizing the pulpal nerves thus interrupting the neural response to pain stimuli[3],[4],[5],[6],[7]. Various other available dentifrices contain desensitizing agents like calcium carbonate, aluminium, calcium phosphate, silicates, strontium chloride, sodium fluoride and zinc chloride which act either by blocking dentinal tubules by the abrasion or by formation of smear layer during brushing or act as protein precipitants[8],[9]. Many of these formulations have been shown to provide measurable reductions in dentin hypersensitivity after two to four weeks of twice daily use and generally several weeks or more to demonstrate maximum effectiveness and achieve maximum levels of pain relief [10],[11],[12]. Their effects are sustained for as long as daily use of the desensitizing toothpaste is continued but may rapidly wear off thereafter. Recently a new dentifrice “Colgate® Sensitive Pro-Relief™” containing Arginine and Calcium carbonate claiming instant and long lasting relief from dental hypersensitivity has become available.
The objective of this clinical study conducted in a group of patients with known dentin hypersensitivity, was to determine the efficacy of Colgate® Sensitive Pro-Relief™ and test the claim of manufacturing company in reducing dentin hypersensitivity of this desensitizing paste containing Arginine and Calcium carbonate, instantly after application as a single in-office application on the affected teeth as claimed by the manufacturing company.
Material And Methods
This clinical study was conducted at B.J.S. Dental College, Ludhiana to clinically evaluate the efficacy of a newly available dentifrice “Colgate® Sensitive Pro-Relief™” on dentin hypersensitivity in providing instant relief from dentin hypersensitivity after a single professional application of the product for 5 minutes. The desensitizing paste contains 8% Arginine and Calcium carbonate as active desensitizing agents.
Inclusion criteria - Eligible study subjects had to be between the ages of 18-70 years and in good general health. They were required to possess a minimum of two hypersensitive teeth with mild - moderate recession as assessed with a blast of air, stream of cold water at 5-10°C temperature and with exploration with an explorer. None of the teeth under evaluation showed mobility, ongoing periodontal disease, pathological migration or had dental restorations or cavities. Subjects with reported history of allergy to any dentifrice were excluded from the study.
Clinical procedure - 61 subjects who met the selection criteria received a baseline evaluation to assess and grade dentin hypersensitivity by air blast, cold water and tactile exploration tests. A trained dental professional applied a pea sized amount of dentifrice being evaluated to the sensitive surfaces of the teeth being tested with a cotton pellet after isolation with cotton rolls. Patients were refrained from rinsing for 4 minutes. After the holding time of 4 minutes, patients were asked to rinse thoroughly with tap water and tactile, cold water and air blast hypersensitivity scoring was repeated.
Clinical Scoring Procedures
Verbal rating scale was used for scoring DHS and patients were told to score degree of hypersensitivity on the following scale.
0 - No hypersensitivity
1 - Mild hypersensitivity
2 - Moderate hypersensitivity
3 - Severe hypersensitivity
Tactile hypersensitivity was assessed using a sharp explorer. For this the tip of a dental explorer was moved approximately at right angle over the tooth being tested using light force similar to the one used for probing and the patients were then asked to grade the pain of hypersensitivity if any.
For evaluation of air blast hypersensitivity, a blast of air was directed from a standard dental unit air syringe on the tooth being evaluated for 1 sec from a distance of 1 cm after covering adjacent tooth surfaces with operator’s fingers.
For assessing cold water sensitivity 5ml cold water at 5-100C was taken in a syringe and slowly flowed in 10 seconds from a distance of 1cm on the tooth being evaluated. The adjacent tooth surfaces were covered by operator’s fingers.
Statistical Methods
Data was collected and tabulated and statistical analysis was performed separately for tactile hypersensitivity, air blast hypersensitivity and cold water hypersensitivity scores. Within treatment groups, comparisons of the baseline versus final hypersensitivity scores were analysed using paired t-test.
Results
Sixty one subjects participated in the study. Throughout the study, there were no adverse effects on the oral soft or hard tissues of the oral cavity as observed by the examiner or reported by the subjects when questioned. The mean pre and post tactile, air blast and cold water hypersensitivity scores are shown in Table 1.
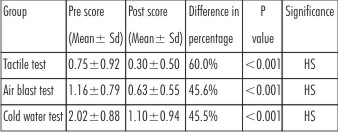 | Table 1 Intragroup comparisons of the mean pre-scores and post-scores of tactile, air blast and cold water tests.
 |
Tactile, air blast and cold water sensitivity scores were recorded before product application and after product application and the comparison was done between the mean pre-operative and post-operative scores.
For tactile hypersenstivity, the mean baseline pre scores were 0.75±0.92 and post-scores were 0.30±0.50. The percentage changes from baseline were 60.0% which is highly significant.
For air blast hypersensitivity, the mean baseline pre-scores were 1.16±0.79 and post-scores were 0.63±0.55. The percentage changes from baseline were 45.6% which is highly significant.
For cold water hypersensitivity, the mean baseline pre scores were 2.02±0.88 and post-scores were 1.10±0.94. The percentage changes from baseline were 45.5% which is highly significant.
Discussion
Dentin/Dentinal hypersensitivity is characterized by short sharp pain arising from exposed dentine typically in response to thermal, evaporative, tactile, osmotic or chemical stimuli which cannot be ascribed to any other form of dental defect or pathology[13],[14],[15]. It is a painful clinical condition that affects 8 to 57% of adult population and is associated with dentin exposure to the oral environment.[16],[17] A recent novel approach for the treatment of DHS is a technology based on Arginine, a natural product, and Calcium carbonate. In 2002, Kleinberg et al. reported the development of this novel desensitizing technology based on the role that saliva plays in naturally reducing dentinal hypersensitivity. Saliva provides calcium and phosphate, which over time occlude and block open dentinal tubules from external stimuli known to cause dentinal hypersensitivity.[18],[19] The technology is proposed to block dentinal hypersensitivity pain by occluding dentinal tubules by using Arginine, which is positively charged at physiologic pH of 6.5-7.5, to bind to the negatively charged dentin surface, which helps attracts a calcium-rich layer from saliva, and infiltrates and blocks dentinal tubules thereby effectively blocking the flow of dentinal fluid through dentinal tubules which is essential for causing DHS as per the widely accepted hydrodynamic theory by Brannstrom. [20],[21]
The purpose of this study was to evaluate the efficacy of the commercially available desensitizing product based on Pro-Argin™ technology “Colgate® Sensitive Pro-relief™” on dentin hypersensitivity. It is demonstrated in this study that as claimed by the company, the effective use of the test product requires less than 1 minute of application time, is very easy to use, and has the advantage of pre-treating suspected hypersensitive areas.
An adult population with history of dentin hypersensitivity was enrolled for participation in this study and tactile, cold water and air blast scores were recorded as baseline hyper-sensitivity values and then after 5 minutes (1 minute dentrifice application and 4 minutes of dentrifice holding time) dentin hypersensitivity was re-evaluated. Significant reductions in dentin hypersensitivity scores i.e., 60.0% reduction in tactile hypersensitivity, 45.6% reduction in air-blast hypersensitivity and 45.5% reduction in cold water hypersensitivity instantly after product application were observed. These results were comparable to the work conducted by Kleinberg et al[19] who reported statistically significant reductions of 58.8% in air blast stimulated hypersensitivity and 64.6% in tactile hypersensitivity for Arginine dentrifice group following a single post-scaling application of the 8% Arginine-Calcium carbonate desensitizing dentrifice. They subsequently conducted a monadic design study to establish duration of the hypersensitivity relief benefit and reported instant hypersensitivity improvements of 71.7% (air blast) and 84.2% (tactile) that were maintained for 28 days after a single application of the product thus validating its use as home application too. A similar clinical study conducted on 390 patients found professional application of Arginine and Calcium carbonate by dentists and dental hygienists in Hong Kong significantly reduced severity of pain in patients with dentine hypersensitivity.[22]
In clinical trials, this product has been found to provide immediate and lasting relief of dentin hypersensitivity for four weeks when it is applied in patients immediately after dental scaling, as a final polishing step during a professional cleaning procedure[23]. Another study demonstrated its effectiveness in relieving dentinal hypersensitivity when applied prior to dental prophylaxis, with a significant reduction in dentinal hypersensitivity postprocedurally[24]. A range of state-of-the-art measurement techniques have been used to establish the mechanism of action of this product e.g., confocal laser scanning microscopy (CLSM) studies etc. These have demonstrated its effectiveness in occluding open dentin tubules[23]. In addition, it was determined through hydraulic conductance testing that these deposits significantly reduced the flow of dentinal fluid in the tubules[25].
Conclusions
The results of this clinical study support the conclusions that – single professional application of the dentrifice containing Arginine and Calcium carbonate (Colgate® sensitive pro-relief™) provides a highly significant instant reduction in dentin hypersensitivity as evaluated with tactile test, air blast test and cold water tests.
The results from this study demonstrate that this desensitizing paste can be used as an in-office modality to provide relief from pre-existing or anticipated dentin hypersenstivity when applied in advance of dental procedures, such as scaling and root planning etc. It seems that this product has the potential to be of great assistance to clinicians in dealing with dentin hypersensitivity as an in office dentinal hypersensitivity controlling agent and home use agent, especially when used prior to pre-existing or anticipated post operative dentinal hypersensitivity.
References
1. Addy M, Urquart E. Dentine hypersensitivity: its prevalence, aetiology and clinical management. Dental Update 1992; 19:407,408,410-412.
2. Addy M. Dentine hypersensitivity: New perspectives on an old problem. Int Dent J 2002; 52:375-6.
3. Tarbet WJ, Buckner A, Stark MM, et al. The pulpal effects of brushing with a 5 percent potassium nitrate paste used for desensitization. Oral Surg1981;600-602.
4. Knight NN, Tryggve L, Clark SM, et al. Hypersensitive Dentin: Testingof procedures for mechanical and chemical obliteration of dentinal tubuli. J Periodontol 1993;64:366-373.
5. Poulsen S, Errboe M, Hovgaard O, et al. Potassium nitrate toothpaste for dentine hypersensitivity(Review). The Cochrane Collaboration 2004, Issue 4, Wiley Publisher.1-11.
6. Nagata T, Ishida H, Shinohara H, et al. Clinical evaluation of a potassium nitrate dentifrice for the treatment of dentinal hypersensitivity. J Clin Peridontol 1994;21 (3):217-21.
7. Schiff T, Dotson M, Cohen S, et al. Efficacy of a dentifrice containing potassium nitrate, soluble pyrophosphate, PVM/MA copolymer, and sodium fluoride on dentinal hypersensitivity: a twelve-week clinical study. J Clin Dent 1994;5 Spec No: 87-92
8. Prati C, Venturi L, ValdrèG, Mongiorgi R (2002) Dentin morphology and permeability after brushing with different toothpastes in presence and absence of smear layer. J Periodontol 73, 183-190.
9. Prati C, Montebugnoli L, Suppa P, ValdrèG, Mongiorgi R (2003) Permeability and morphologyof dentin after erosion induced by acidic drinks. J Periodontol 74, 428-436.
10. Cummins D: Dentin Hypersenstivity: From diagnosis to breakthrough therapy for everyday sensitive relief. J Clin Dent 20(Spec Iss):1-9, 2009
11. Millers, Truong T, Heu R, Stranick M. Bouchard D, Gaffar A: Recent advances in stannous fluoride technology: Antibacterial efficacy and mechanism of action towards hypersensitivity. Int Dent J 44(suppl):83-98,1994
12. Walters PA: Dentin hypersensitivity: A review. J Contemp Dent Pract 6:107-117,2005
13. Canadian Advisory Board on Dentine Hypersensitivity. Consensus-based recommendations for the diagnosis and management of dentine hypersensitivity. J Can Dent Assoc.2003;69:221-6
14. Que K, Ruan J, Fan X, Liang X, Hu D. A multi-centre and cross-sectional study of dentine hypersensitivity in China.J Clin Periodontol.2010;37:631-7
15. Rees JS. The prevalence of dentine hypersensitivity in general practice in the UK. J Clin Periodontol.2000;27:860-5
16. Markowitz K, Pashley DH (2007) Personal reflections on a sensitive subject. J Dent Res86,292-295
17. Addy M (2000) Dentine hypersensitivity:definition, prevalence, distribution and aetiology. In: Tooth wear and sensitivity; clinical advances in restorative dentistry ,Addy M, Embery G, Edgar WM, Orchardson R eds, Martin Dunitz,London,239-248l
18. Panakos F, Schiff T,Guigon A. Dentin hypersensitivity: Effective treatment with an in-office desensitizing paste containing 8% arginine and calcium carbonate .Am J Dent. 2009;22(Special Issue):3A-7A
19. Kleinberg I.Sensitat: A new saliva-based composition for simple and effective treatment of dentinal hypersensitivity pain. Dent Today.2002;21:42-7
20. Brannstrom M. Dentin sensitivity and aspiration of odontoblasts. J Am Dent Assoc.1963;66:366-70
21. Cummins D. Dentin hypersensitivity: From diagnosis to a breakthrough therapy for everyday sensitive relief. J Clin Dent. 2009;20(Special Issue):1-9
22. Chu CH, Lui KS ,Lau KP, Kwok CM, Huang T. Effects of 8% arginine desensitizing paste on teeth with hypersensitivity .J Dent Res 2010,89(Spec Issue A)(Submitted on Feb 5,2010)
23. Schiff T, Delgado E ,Zhang YP, et al. Clinical evaluation of the efficacy of an in –office desensitizing paste containing 8% arginine and calcium carbonate in providing instant and lasting relief of dentin hypersensitivity.Am J Dent.2009;22(Spec Issue): 8A-15A
24. Hamlin D, Phlean Williams E, Delgado E, et al. Clinical evaluation of the efficacy of a desensitizing paste containing 8% arginine and calcium carbonate for the in-office relief of dentin hypersensitivity associated with dental prophylaxis. Am JDent. 2009;22:16A-20A
25. Petrou I, Heu R, Stranick M, et al. Abreakthough therapy for dentin hypersensitivity:dental products containing 8% arginine and calcium carbonate work to deliver effective relief of sensitive teeth.J Clin Dent.2009;(Spec Iss);23-31
|